

Adjuvant CDK4/6 Inhibitors Still Under Debate: Preparing for the NATALEE and monarchE Updates at ESMO 2025.
With nearly 40% of patients newly diagnosed with breast cancer potentially eligible, the stakes are high.

The ESMO 2025 conference will open on Friday, October 17th, with updates on both trials: a 5-year update from NATALEE, and the first presentation of the survival benefit from MonarchE, as announced in a recent press release.

Why talk about the NATALEE and MonarchE updates at ESMO?
1 - One of the largest potentially eligible patient populations in oncology.
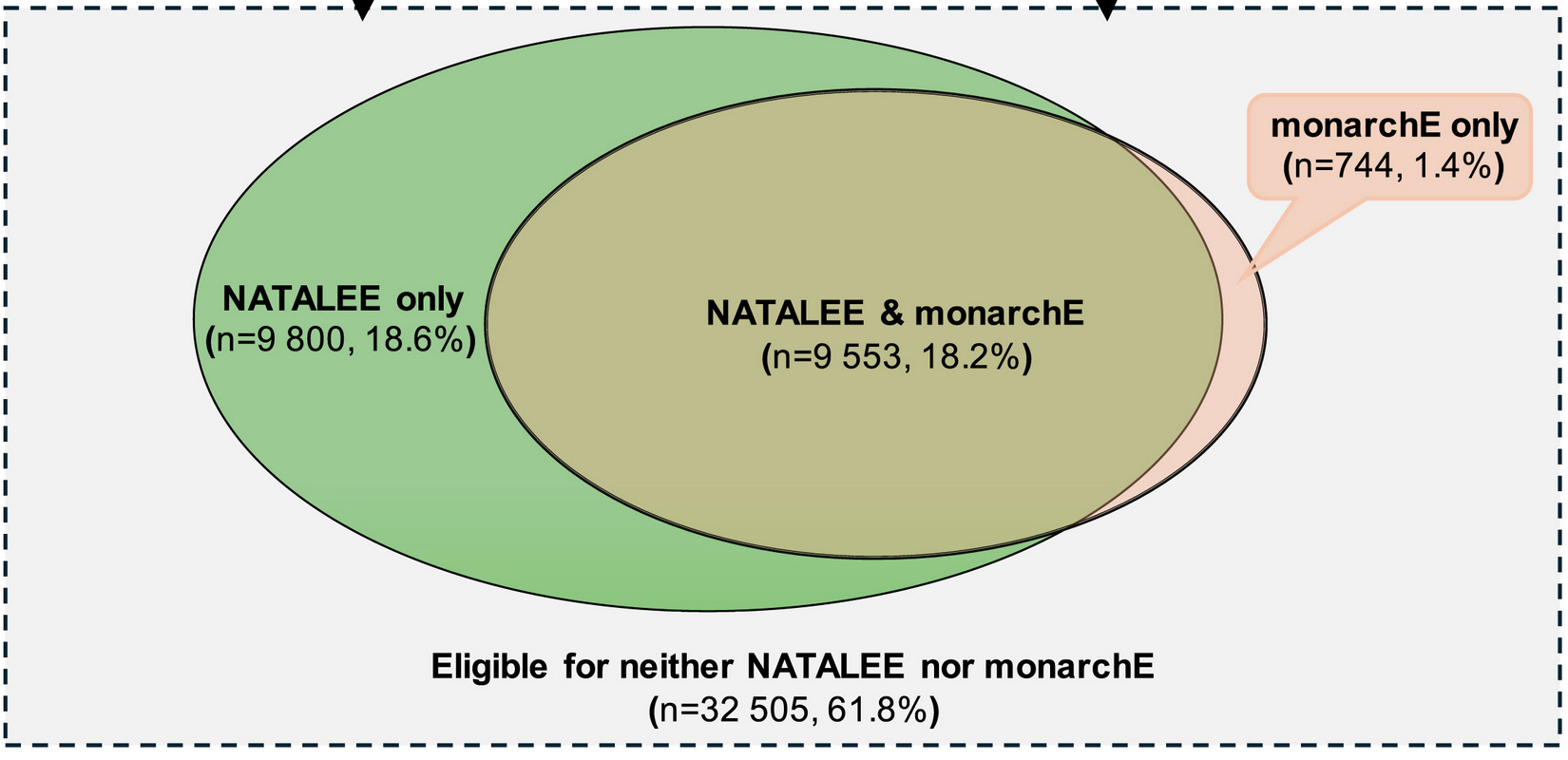
About 20% of patients with HER2-negative, hormone receptor–positive early breast cancer — one of the most common cancers worldwide in terms of incidence — could be eligible for the MonarchE trial, which evaluates 2 years of adjuvant abemaciclib and focuses on those at higher risk. With broader eligibility criteria, up to 38% of patients could be eligible for the NATALEE trial — 3 years of adjuvant ribociclib — largely overlapping with the MonarchE population (figure below from Swedish data).
2 - Yet, results are still under debate.
The MonarchE trial, the first phase 3 study to demonstrate a significant improvement in iDFS in this setting, was examined by Meirson et al. (here), where the authors concluded: “Adjuvant abemaciclib should not be prescribed to women with high-risk, oestrogen-receptor positive breast cancer.”
Soon after the NATALEE publication, we questioned the validity of its results in the European Journal of Cancer, mainly due to the possibility of informative censoring (here, caption below, + watch my talk in Cambridge here).
More recently, a paper by Tannock et al. also advised to “not recommend” adjuvant CDK4/6 inhibitors (here).

3 - The subject is highly topical — and the stakes are high
With two new publications in September and a press release announcing an overall survival benefit in MonarchE, the topic is particularly timely. Given the large eligible population, the differences between the two trials and the debate surrounding them are even more intense.
The 4-year update of the NATALEE trial was just published on September 25, 2025, in JAMA Oncology — adding to an already dense flow of data only three weeks before the expected 5-year update at ESMO.
In addition, Fabio Conforti et al. published on September 17, in the Journal of Clinical Oncology, an article advocating for the use of CDK4/6 inhibitors in the adjuvant setting, including sensitivity analyses on censoring.
However, the core point of our analysis has been overlooked in their analysis, as I will show.
The value of digitized curves.
In their article, Fabio Conforti et al. contest the sensitivity analyses performed by our group and others using data reconstructed from digitized survival curves.
First and foremost, I’m pleased that the authors conducted sensitivity analyses using digitized curves, as this underscores the value of such approaches. From these digitized curves, one can reconstruct pseudo–individual patient data (pseudo-IPD), which allow for the performance of various sensitivity analyses.
Even though these data can only be estimates, they remain highly valuable, as they enable near real-time sensitivity analyses as soon as a new Kaplan–Meier curve is presented — whether at a conference or in a publication.
Here, I will focus on the NATALEE sensitivity analysis.
Sensitivity analyses should consider “reasons” for censoring
Censoring should occur at random. If not, and if the reason for censoring is related to the allocated therapy, then informative censoring can occur. The two main reasons for informative censoring are the following:
Censoring due to toxicity: Frailer patients — those who are also most at risk of experiencing the event — may be censored in relation to toxicity (not directly, but for example, by not returning for evaluations, withdrawing consent, etc.), thus artificially favoring the more toxic arm. This is more likely to happen in more toxic experimental arms.
Censoring due to disappointment: Healthier patients — those able to seek options outside the trial and less at risk of experiencing the event — may be disappointed with their treatment allocation, and withdraw or be censored in excess, thus artificially penalizing the group they were initially assigned to, since frailer patients remain. This is more likely to happen in control arms.
If some of the (1) toxicity-driven censoring occurs in the experimental arm, and some of the (2) disappointment-driven censoring occurs in the control arm, informative censoring can still be present even with equal rates of censoring.
We described and illustrated this concept in a European Journal of Cancer publication (here, see caption below).
Fabio Conforti et al. did not perform such an analysis. They only focused on the imbalance in censoring, and modified the outcomes of patients censored “in excess” in one arm as compared to the other. In other words, they did not account for the possibility that different reasons for censoring could have affected the two treatment arms differently, which was the core of our analysis.
However:
some level of early toxicity-driven censoring could have occurred in the experimental arm, and
some level of early disappointment-driven censoring could have occurred in the control arm.
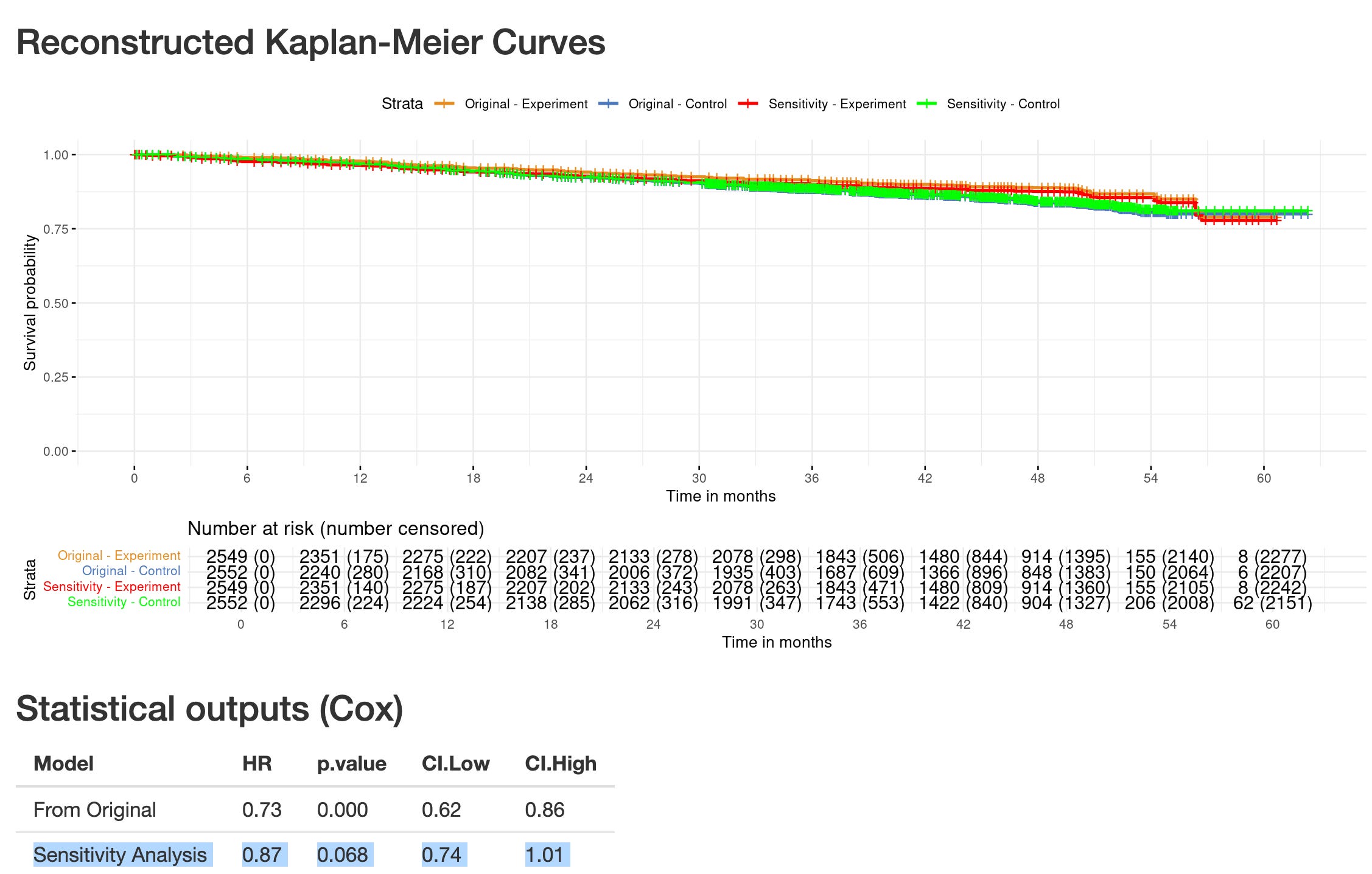
If we select 20% of censored patients in each arm over only the first 6 months, and apply this analysis, the iDFS gain is no longer significant (see caption below from https://www.timotheeolivier-research.com/breaking-ice, also available by selecting “NATALEE-4yiDFS-JAMAOnc” in the Web App).
What to expect from the trials’ updates?
1 - NATALEE
I don’t expect much from the 5-year updates of NATALEE. The 4-year update was just published in JAMA Oncology, and only three weeks later those data already feel outdated — with new results expected at ESMO. The number needed to treat (NNT) may fluctuate, but this doesn’t change the main points we raised right after the original publication.
2 - MonarchE
From MonarchE, what I hope to see is the post-protocol access to CDK4/6 inhibitors. This is a key element to consider when a survival gain is reported. If patients in the control group of MonarchE who developed metastatic recurrence had limited access to CDK4/6 inhibitors, then any observed survival benefit would have little validity in our daily practice, where first-line or second-line CDK4/6 inhibitors are the standard of care since years in the metastatic setting. (More on the importance of post-protocol care here.)
Also, the censoring pattern in the survival analysis will be a point of interest, as informative censoring — too often overlooked — can also affect overall survival.
Of course, both trials will come with exclusive BREAKING-ICE App© sensitivity analyses — stay tuned for the insights!