

Sham Controls and Tumor Treating Fields: Does the Ethical Argument Hold?
Our new paper published in the European Journal of Cancer highlight current limitations regarding the efficacy of TTFs in oncology.


Today, we are covering our new work just published in The European Journal of Cancer, entitled “Tumor treating fields: Will the evidence gap ever be filled?”. We thank our co-authors Sruthi Ranganathan, Susannah Ellsworth, and Alessandro Hammond!
What is a sham-control?
When you take a pill, part of the benefit may come from placebo effects. The same can be true for medical devices. For example, with a wearable that you have to put on for 18 hours a day, expectations, routine, support and coaching may drive the effect. To show that a device really works, it is important to blind patients and investigators in a sham-controlled randomised trial. (more on this here, and here).
Sham controls are like placebo controls, but instead of a placebo drug, patients receive a version of the device or procedure without the active therapeutic component.
Placebo effects from devices can be even greater than those from pills. And a device can come with extra-care potentially influencing patients’ outcomes.
Does the Ethical Argument Hold?
Tumor treating fields (TTFs) deliver low-intensity electric fields through a device connected to adhesive pads placed on the patient’s skin, aiming to exert direct antitumor activity mainly through mitotic disruption, with additional hypothesized effects on DNA damage, oxidative stress, immune activation, autophagy, and blood–brain barrier permeability. However, the biologic plausibility remains insufficiently validated. Rigorous human in vivo dosimetry is lacking, clinicopathologic validation is limited, and effects on normal proliferative tissues are not clearly observed.
Nonetheless, some TTFs trials have reported a survival benefit, these are the EF-14 trial in glioblastoma, the LUNAR trial in lung cancer, and the PANOVA-3 trial in pancreatic cancer.
We posit that without a sham-control trial, the exact contribution of the electric fields cannot be isolated :
“In oncology, where progression-free survival (PFS) and overall survival (OS) are not subjective outcomes, sham control could be seen as unnecessary, or even unethical. This would overlook a key component of TTF use: the co-interventions and the intensity of care associated with the device. With TTFs, patients and their families not only receive the device, but also additional support and infrastructure around its use, such as 24/7 assistance, home deliveries, and increased home-based interactions for device management, including regular array changes.”
For instance, there are a numbers of trials showing that early palliative care improved survival in patients with advanced cancer. Moreover, the magnitude of benefit reported in those trials is comparable with that reported in TTFs trials reporting a survival gain, like in glioblastoma in the EF-14 trial. (see figure below).
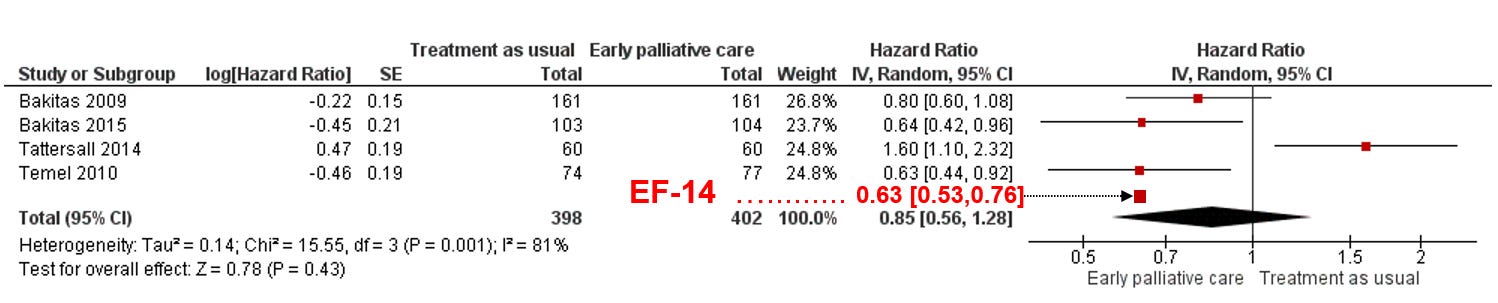
In other words, it is not excluded that the survival benefit seen with TTFs may have been driven by the extra-care associated with the device, rather than by the electric fields themselves.
“In order to isolate the specific effect of TTFs from that of the care accompanying the device use, the most rigorous approach would be a sham-controlled trial using a device identical in appearance but not delivering electric fields. Yet, throughout TTF development, no trials have used a sham control. One might argue that they would pose an ethical dilemma: how could we expose patients to the physical burden of TTFs, without any active intervention, without the electric fields? However, this ethical critique fails in two ways. First, if that burden cannot be ethically justified for control-arm patients, then we should also question whether it is appropriate to impose the same burden on patients in the experimental arm. Second, without a sham-controlled trial, it is possible we are exposing thousands of patients to a therapy that may have no benefit in and of itself - an uncertainty that raises even greater ethical concerns.”
Suboptimal control arms and changes in sample sizes
We identified six completed randomized trials studying TTFs. A first concern is that 3 out of 6 used suboptimal control arm. (see Table 1). Detailed explanations on each of these trial and their control group are available in our manuscript.
“A survival gain observed against a weaker comparator may not persist when compared with the best available care.”
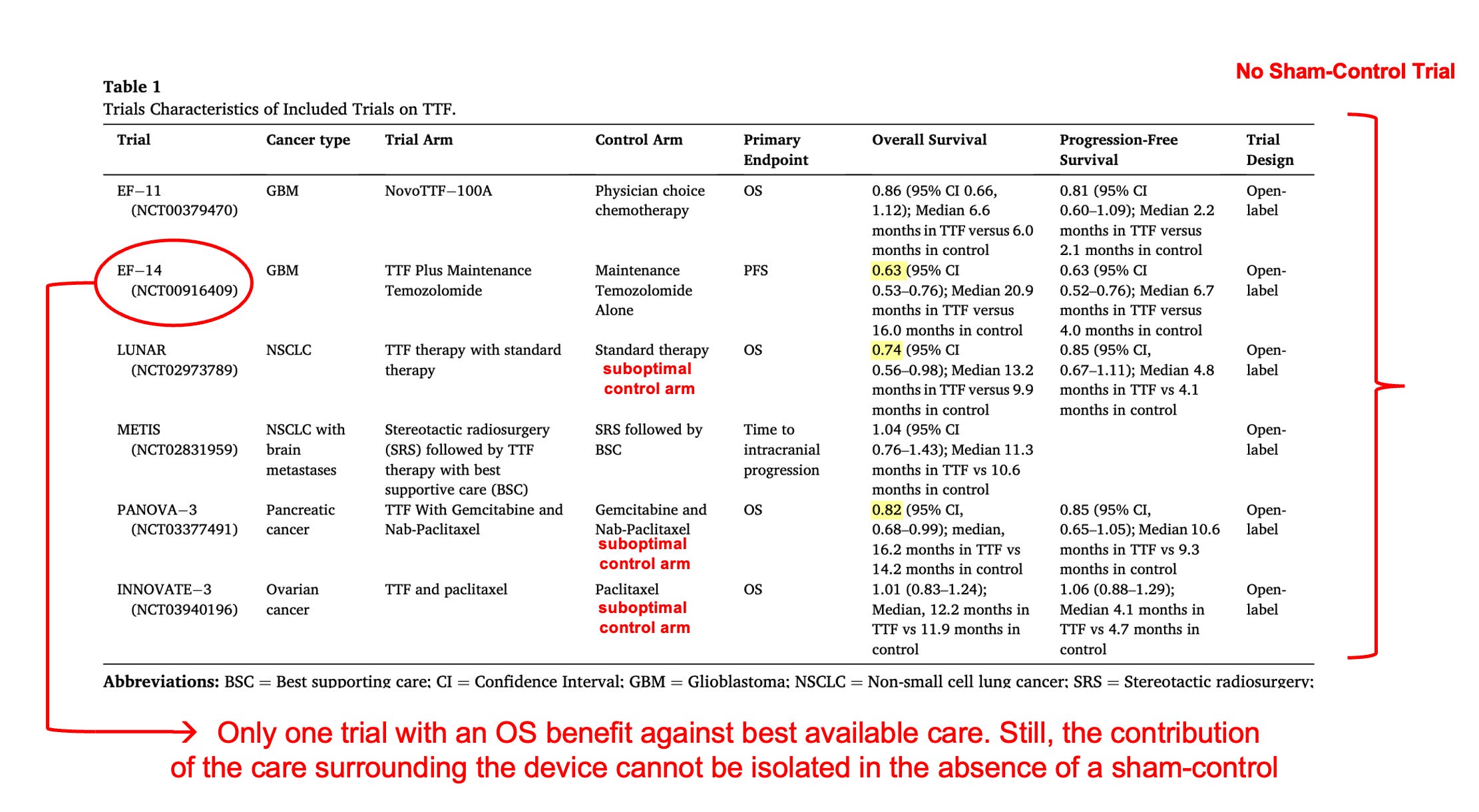
Another concern relates to sample size modifications. In one trial, LUNAR, the sample size was lower than initially planned, raising the risk of a spurious finding. In another trial, PANOVA-3, the final sample size was greater than originally planned, with final results at the cusp of significance. Was this increase planned? What was the explanation? Would the results have remained significant had the sample size been as originally planned?
Without regulatory requirements, evidence may never be delivered
First, we noted : “TTFs occupy a uniquely isolated evidentiary position: the entire pivotal evidence, implementation infrastructure, and post-market data are concentrated within a single sponsor. This concentration is not inherently disqualifying, but it amplifies the importance of even more careful scrutiny.”
In both the United States and Europe, regulators allow greater flexibility for medical devices than for drugs. In the US, approval is based on “reasonable assurance of safety and effectiveness” and “least burdensome” principles, while in Europe devices can obtain CE marking without requiring sham-controlled trials. Regulators rely in part on post-market clinical follow-up (PMCF) to address remaining uncertainties, but in practice these data are often not publicly available or incomplete. As a result, devices can enter clinical practice with substantial uncertainty regarding their clinical benefit, and the evidence gap may not ever be closed.
Check out our full manuscript here for deeper insights, as well as a prior publication on the LUNAR trial that was published with Vinay Prasad (here).
 | A guest post by
|