

Additional Insights Into Early Daraxonrasib Data
Let’s take a deep dive into the early-phase data on daraxonrasib in patients with metastatic pancreatic cancer, just published in the New England Journal of Medicine.
Daraxonrasib is making headlines. A few weeks ago, a press release reported positive phase 3 results from the RASolute 302 trial in second-line metastatic pancreatic cancer, with particular emphasis on a secondary endpoint: overall survival in all patients. Full data are expected at the upcoming American Society of Clinical Oncology annual meeting. See my previous post for what to watch for when the full data are presented (here).
Now, the phase 1b/2 data have finally been published in The New England Journal of Medicine.
A quick recap: daraxonrasib inhibits the active RAS(ON) form. Because even RAS wild-type tumors may depend on RAS activation, this provides the rationale for investigating daraxonrasib beyond RAS-mutant populations.
Response rates: which number matters?
In most early phase data, response rates are not the primary endpoint, which is often safety measures. In RMC-6236-001, this was the case, yet the abstract emphasizes the most favorable response-rate metrics.
“In a subgroup of 26 patients with RAS G12 mutations who were treated with second-line daraxonrasib at a dose of 300 mg, an objective response to therapy was reported in 35% (95% confidence interval [CI], 17 to 56).[…] Among the 38 patients with RAS G12, G13, or Q61 mutations, 29% (95% CI, 15 to 46) had an objective response.”
However, there are many response rates in RMC-6236-001
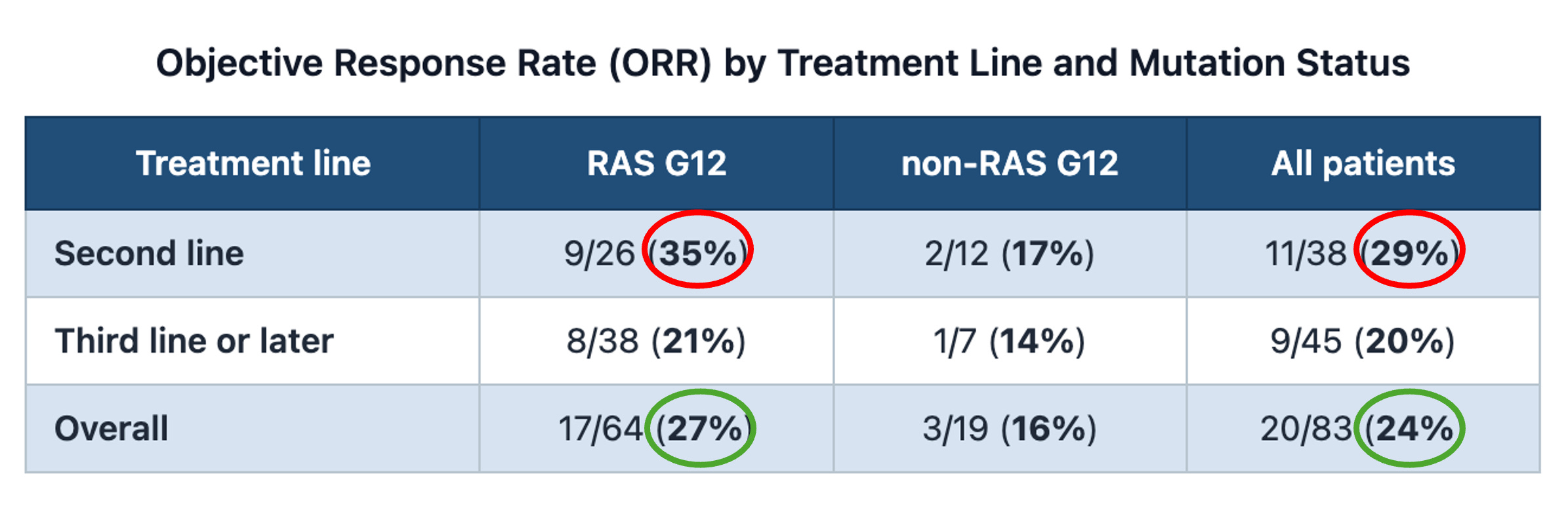
In small phase 1/2 trials, with highly selected patients, the relevance of breaking down the results according to the line of therapy is not as obvious as in larger phase 3 trials.
The response rate in the overall treated population (24%), together with the breakdown by RAS status (with 27% in G12-mutant population), are both highly relevant, yet not explicitly reported as standalone values by the authors.
Comparison with other studies
Here is an informal contextualization with prior selected trials in a comparable setting (disclaimer, this is not a systematic review!).
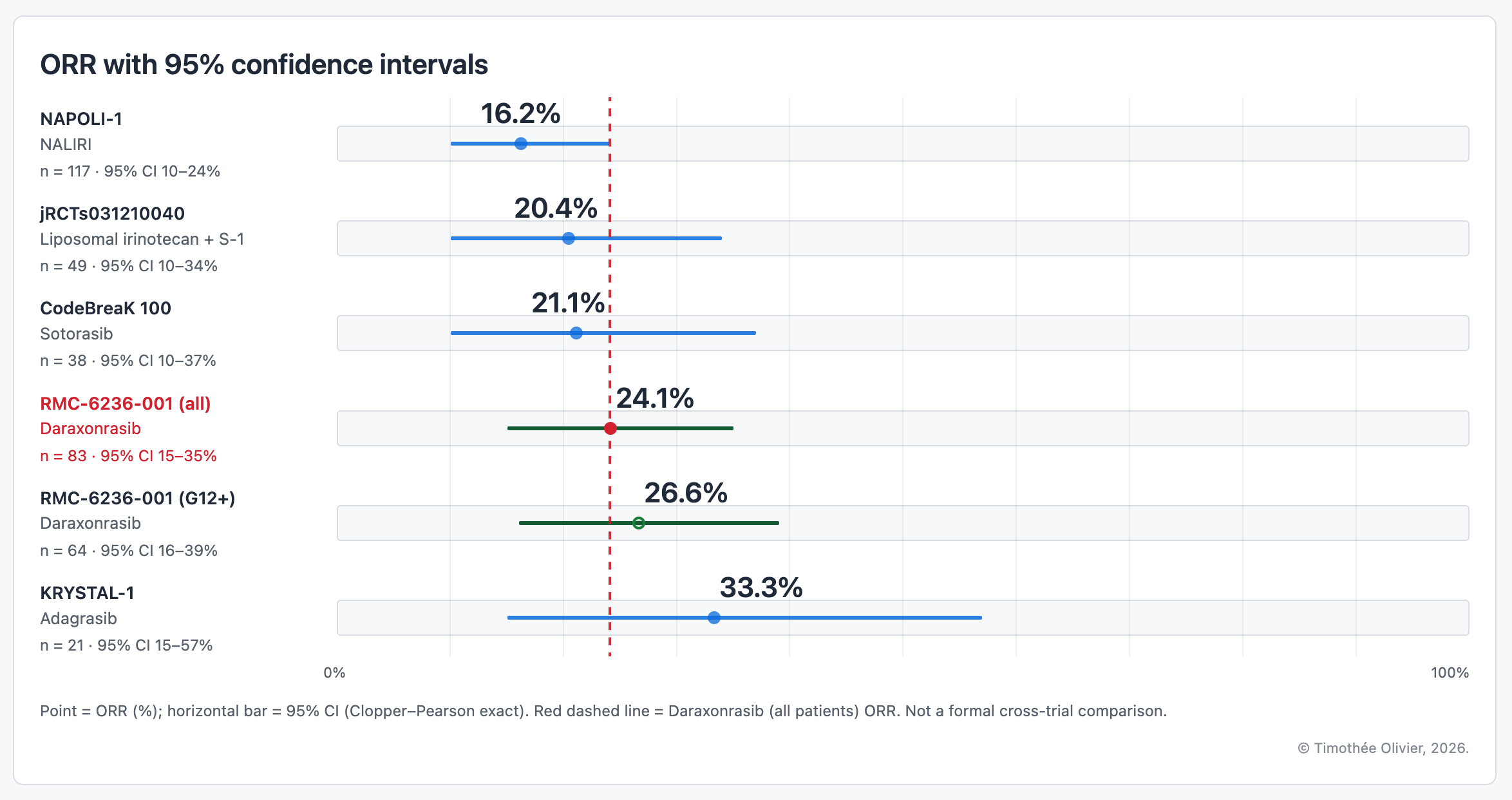
In this figure, ORRs are reported for the overall study population of each trial, with no breakdown according to line of therapy.
Importantly, the characteristics of the populations included varied across studies. In NAPOLI-1, 53% of patients received NALIRI as second-line therapy in the metastatic setting, 34% as later-line treatment, and 13% had previously received systemic therapy, although not in the metastatic setting. In the Japanese study (jRCTs031210040), all patients had metastatic pancreatic cancer refractory to first-line gemcitabine-based chemotherapy, with no further detailed breakdown reported. In CodeBreaK 100, 55% of patients had stage IV disease at initial diagnosis, and all patients had metastatic disease at enrollment; 79% had received two or more prior lines of therapy. In KRYSTAL-1, 76% of patients had received two or more lines of systemic therapy before enrollment.
Bottom line: early signals of activity, but still within the historical ballpark
The much awaited phase 3 RASolute 302 trial will provide more precise estimates of response rates in a larger and more homogeneous population (second-line therapy in the metastatic setting).
Survival?
Interpreting survival data from single-arm early-phase trials should be done very cautiously. In order to receive multiple lines of therapy, patients need to be fit enough and likely have a more indolent tumour biology, unlike rapidly progressing cancers that can sometimes lead to death before any therapy can even be administered.
As a result, and this is somehow counterintuitive, we may see longer survival in later-line early-phase trials than in first-line phase 3 trials.
An example is durvalumab in urothelial carcinoma. In an early phase I/II study conducted mostly in previously treated/post-platinum patients, median OS was reported at 18.2 months. However, in the first-line phase III DANUBE trial, durvalumab monotherapy showed a shorter median OS: 14.4 months in the PD-L1–high population and 13.2 months in the ITT population.
As such, caution is warranted when drawing conclusions from PFS or OS data from early-phase trials.
Toxicity in the 300 mg cohort: more details are needed.
Below is a focus on the 300 mg cohort, the dose chosen for phase 3 trials.
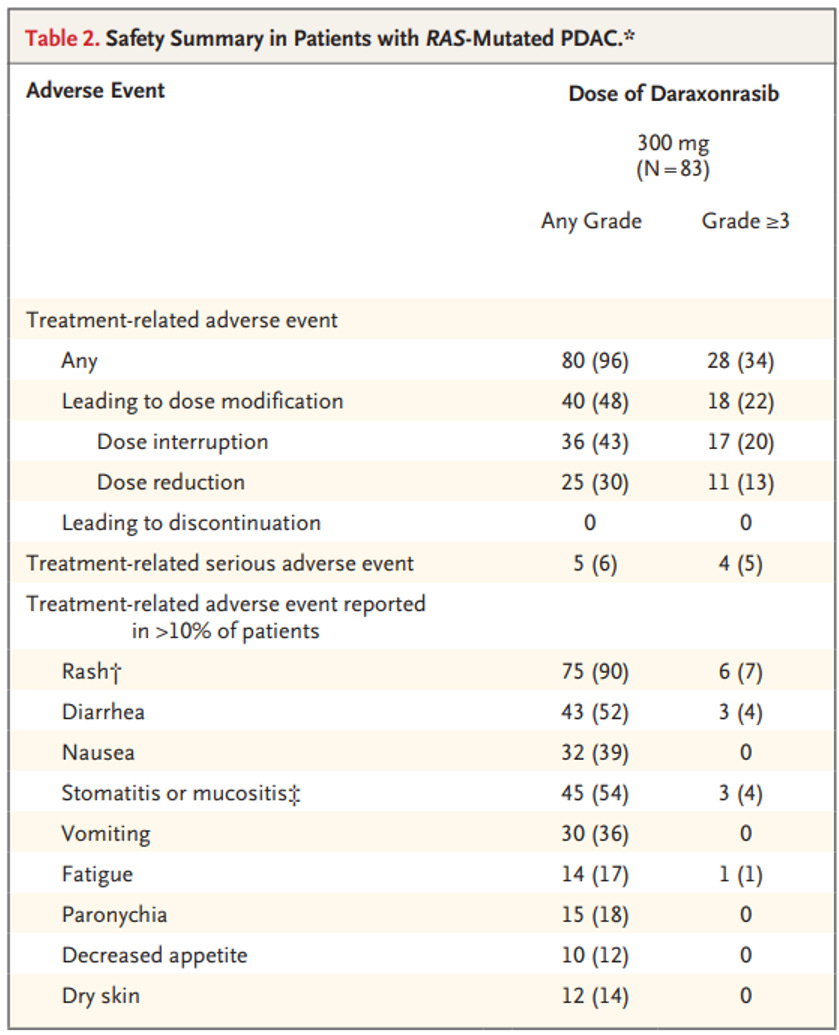
There is a striking difference between the rate of grade ≥3 treatment-related adverse events (TRAEs, 34%) and the summed frequency of individual grade ≥3 TRAEs occurring in >10% of patients (13%).
Even though Table S2 reports additional safety data, it still leaves 10 patients with undocumented grade ≥3 TRAEs in the 300 mg cohort, since only events leading to dose modification and occurring in ≥2% of patients were described.
Toxicity was not dominated by a single adverse event, but rather distributed across multiple less frequent toxicities. However, the type of the remaining unreported grade ≥3 TRAEs (12% of patients) is not described.
Enthusiasm should not hamper cautious appraisal
Daraxonrasib shows unquestionable early activity in metastatic RAS-mutated pancreatic cancer. However, the data remain within a range comparable to that observed in other studies. Toxicity is a significant concern, and grade ≥3 toxicities are not fully detailed.
While we can understand the natural enthusiasm in such a poor-prognosis setting, we should at the same time try not to deviate from an objective and thorough appraisal of the data. Looking forward to the upcoming ASCO presentation! (See my previous post on what to look for in the full data presentation.)
great context ... thank you